Content Menu
● Who Is at Risk for Penicillin G Procaine Anaphylaxis?
● Recognizing the Symptoms of Anaphylaxis
● Immediate Response: Step-by-Step Protocol
● Hospital Management: Advanced Care Protocols
● Long-Term Management and Prevention
● Manufacturing, Distribution, and Regulatory Considerations
● How to Select Alternatives to Penicillin G Procaine
● Industry Innovations: Enhancing Product Safety
>> 1. What is the most effective first-line treatment for anaphylaxis caused by Penicillin G Procaine?
>> 2. Are alternative antibiotics available for penicillin-allergic patients?
>> 3. Can patients with penicillin allergy safely receive cephalosporins?
>> 4. Is it possible to desensitize patients to penicillin if necessary?
>> 5. What steps can manufacturers take to minimize risks?
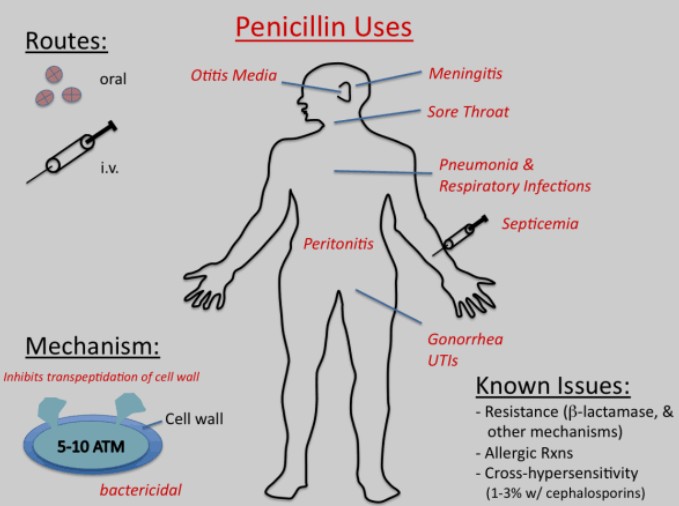
Penicillin G Procaine is a critical antibiotic in clinical practice, widely used for treating moderate to severe infections caused by susceptible bacteria. Despite its benefits, a small subset of patients may experience severe hypersensitivity reactions, particularly anaphylaxis, which requires rapid intervention to prevent fatal outcomes. Understanding risk factors, symptom recognition, emergency protocols, and long-term management is essential for manufacturers, distributors, healthcare professionals, and end users dealing with penicillin-based pharmaceuticals.[2][3][4]
Anaphylaxis represents the most dangerous allergic response to Penicillin G Procaine and other beta-lactam antibiotics. It is a rapid-onset, multisystem immune response, typically occurring within minutes to an hour after drug exposure. This reaction is characterized by widespread histamine release from mast cells and basophils triggered by antigen-bound IgE antibodies. Effects include sudden drop in blood pressure, airway constriction, skin and mucosal swelling, and possibly death if left untreated.[3][5][8][2]
While less common, sub-acute reactions may occur days after treatment starts or following repeat exposure, manifesting as urticaria, fever, or arthralgias due to IgG-mediated complement activation. Both acute and sub-acute forms highlight the unpredictability of penicillin hypersensitivity, even in those previously tolerant to the drug.[4][5]
Patients with a history of IgE-mediated allergy—such as prior episodes of drug anaphylaxis, hives, angioedema, or respiratory compromise—are at highest risk. Parenteral administration, including the intramuscular route for Penicillin G Procaine, increases risk compared to oral forms. Individuals with multiple allergies or atopic conditions (eczema, asthma) also have heightened sensitivity. Notably, sensitivity is not always permanent; individuals may lose or regain allergic disposition over time.[1][5][3]
Before initiating therapy, a thorough review of the patient's drug, food, and environmental allergy history is mandatory. Cross-reactivity between penicillins and cephalosporins, while rare, may occur, justifying caution in those with histories of multiple beta-lactam reactions.[1][3]
Anaphylactic reactions unfold quickly. Classic symptoms include:
- Skin and Mucosal Changes: Sudden appearance of hives, swelling around eyes and lips (angioedema), or flushing.
- Respiratory Compromise: Shortness of breath, wheezing, stridor, chest tightness, difficulty swallowing, or voice changes.
- Cardiovascular Instability: Dizziness, fainting, rapid or weak pulse, hypotension, or shock.
- Gastrointestinal Distress: Abdominal pain, vomiting, diarrhea.[9][10][11]
Symptoms tend to escalate rapidly, with respiratory and circulatory collapse possible in severe cases. Without intervention, anaphylaxis can be fatal within minutes.[8][9]
Every second counts in anaphylactic emergencies. The recommended steps are:
1. Administer Epinephrine IM Immediately
- Deliver 0.3 to 0.5 mg epinephrine into the outer thigh muscle using a pre-loaded auto-injector or manual syringe.
- Repeat every 5–15 minutes if symptoms persist, up to two additional doses.[2][3][9]
2. Activate Emergency Medical Services
- Call 911 or your local emergency response number and specify a suspected drug-related anaphylactic reaction.[12][9]
3. Patient Positioning
- Lay the patient flat with legs elevated unless breathing is compromised, in which case the patient should sit up to ease respiration.
- Pregnant patients should be placed on their left side to reduce vena cava compression.[13][12]
4. Supportive Measures
- Monitor pulse, breathing, and consciousness. Prepare for CPR or airway management if needed.
- Administer high-flow oxygen, establish large-bore IV access, and begin rapid infusion of normal saline (1–2 liters bolus).[13][2]
5. Adjunctive Medications
- Administer H1 antihistamines (e.g., diphenhydramine IV) and H2 blockers (e.g., ranitidine IV).
- Give IV glucocorticoids such as 125 mg methylprednisolone to reduce inflammation.[2]
- For bronchospasm: Consider nebulized albuterol.[2]
6. Hospital Admission and Monitoring
- All patients experiencing moderate to severe anaphylaxis require hospital admission and close monitoring for recurrent symptoms and delayed reactions.[13][2]
When the patient reaches the hospital:
- Maintain continuous cardiac and oxygen monitoring (telemetry).[2]
- Re-administer epinephrine if necessary, using IV infusions for refractory cases (0.1 mcg/kg/min).[13][2]
- Aggressive fluid replacement for persistent hypotension; additional vasopressors may be considered for shock.
- Monitor airway; intubation may be required in severe cases.[3]
- Observe for at least several hours post-symptom resolution; biphasic reactions can occur.
For patients with milder symptoms (isolated skin rashes), antihistamines alone may suffice, but observation is prudent.[2]
Consistent preventive strategies protect against future allergic disasters:
1. Allergic Status Documentation
- Maintain detailed allergy history in medical records and communicate across all healthcare interactions.[1][3]
2. Medical Alert Identification
- At-risk patients should wear a visible medical alert bracelet specifying penicillin allergy, recognized internationally by emergency medical teams.[14][15]
3. Epinephrine Auto-Injector Readiness
- Prescribe at least two auto-injectors for immediate access and train the patient, family, and colleagues in their correct use.[8][12]
4. Specialist Consultation and Allergy Testing
- Refer for allergy work-up, including skin tests and, if appropriate, supervised oral or parenteral challenge tests.[14][1]
5. Education and Emergency Plan
- Educate all household and workplace contacts on recognizing early symptoms and activating emergency protocols. Prepare written action plans, especially in clinical and industrial settings.
6. Desensitization Procedures
- Controlled drug desensitization can be performed only when alternative antibiotics are unavailable or unsuitable. This protocol, managed by allergists in hospital settings, involves giving tiny doses of penicillin at safe intervals to promote tolerance, but is contraindicated in non-IgE mediated reactions such as Stevens-Johnson syndrome (SJS) or toxic epidermal necrolysis (TEN).[2]

For companies manufacturing or supplying penicillin G procaine:
- Risk Disclosure: Clearly state hypersensitivity risks and contraindications in product labeling, inserts, and promotional materials; comply with pharmaceutical regulatory guidelines.[7][3]
- Customer Training: Provide comprehensive education for end users, especially pharmacists and clinicians, on allergy assessment and emergency protocols.
- Post-Marketing Surveillance: Continuously monitor reported allergic reactions and update safety communications accordingly.
- Quality Control: Ensure consistent formulation, accurate dosing, and reliable safety packaging. Engage with global standards and adapt to international market requirements.
Patients with confirmed IgE-mediated allergies must avoid further beta-lactam exposure except under specialist advice. Alternatives for most infections include:
- Macrolides (e.g., erythromycin)
- Clindamycin
- Tetracyclines
- Fluoroquinolones
Selection depends on infection type, bacteriological test results, and individual risk profiles. For those at low risk (non-urticarial rash, remote history, etc.), third-generation cephalosporins may be safe if closely monitored.[1][2]
In rare, essential situations where penicillin is the only option, controlled desensitization should be instituted under specialist supervision. Most acute reactions, however, preclude further penicillin therapy on safety grounds.[1][2]
Modern pharmaceutical companies frequently adopt advanced measures to mitigate hypersensitivity risks:
- Pre-filled Epinephrine Kits bundled with injectable antibiotics
- Automated Patient Risk Screening platforms prior to prescribing or product release
- Global Training Modules for hospital staff and primary care providers
- Regular Product Audits and adherence to strict recall protocols if allergic risks emerge
These innovations strengthen brand reputation, protect patient welfare, and ensure regulatory compliance worldwide.
Anaphylactic reactions to Penicillin G Procaine remain a life-threatening emergency demanding expert recognition and immediate intervention. Healthcare professionals, manufacturers, and distributors must work together to deliver prompt patient care, robust product safety, and global educational outreach. Responsible manufacturing and marketing practices safeguard end users and help build trust and reliability for OEM pharmaceutical delivery. To explore custom manufacturing, high-risk product design, or partner on allergy-safe pharmaceutical solutions, contact our biotechnology and medical device experts at supplybenzocaine.co.uk—your trusted source for safe, innovative OEM development in drug, device, and healthcare markets worldwide.[5][4][7][9][3][1][2]

Epinephrine, given intramuscularly, is the only validated immediate intervention and should be administered without delay.[9][3][2]
Yes, macrolides, clindamycin, tetracyclines, and fluoroquinolones are commonly used alternatives. Selection depends on infection type and individual risk factors.[1][2]
In most cases, yes, particularly with third-generation cephalosporins if the patient has a low-risk allergy profile. However, specialist advice is recommended for those with severe or recent IgE-mediated reactions.[1][2]
Desensitization protocols allow controlled use of penicillin in hospital settings when no alternative drug is effective. This must be performed by specialists and is contraindicated in non-IgE mediated severe adverse reactions.[2]
Include clear labeling about allergic risks, provide educational materials, train clients in emergency protocols, and maintain robust post-market surveillance and safety audits.[7][3]
[1](https://www.cdc.gov/std/treatment-guidelines/penicillin-allergy.htm)
[2](https://www.ncbi.nlm.nih.gov/books/NBK459320/)
[3](https://labeling.pfizer.com/showlabeling.aspx?id=718)
[4](https://www.mayoclinic.org/drugs-supplements/penicillin-g-benzathine-and-penicillin-g-procaine-intramuscular-route/description/drg-20452194)
[5](https://pmc.ncbi.nlm.nih.gov/articles/PMC3255391/)
[6](https://www.aaaai.org/Aaaai/media/MediaLibrary/PDF%20Documents/Practice%20and%20Parameters/Practical-Guidance-for-the-Evaluation-and-Management-of-Drug-Hypersensitivity-2020.pdf)
[7](https://reference.medscape.com/drug/penicillin-g-procaine-999572)
[8](https://en.wikipedia.org/wiki/Anaphylaxis)
[9](https://my.clevelandclinic.org/health/diseases/8619-anaphylaxis)
[10](https://my.clevelandclinic.org/health/diseases/16624-penicillin-allergies)
[11](https://www.healthline.com/health/anaphylaxis-pictures)
[12](https://www.nhs.uk/conditions/anaphylaxis/)
[13](https://www.allergy.org.au/hp/papers/acute-management-of-anaphylaxis-guidelines)
[14](https://www.aaaai.org/tools-for-the-public/video-library/allergy-videos/penicillin-allergy-testing-video)
[15](https://www.mayoclinic.org/diseases-conditions/penicillin-allergy/symptoms-causes/syc-20376222)
Hot tags: Anaphylaxis Treatment, Penicillin Allergy Management, Emergency Response Anaphylaxis, Epinephrine Administration, Allergic Reaction Symptoms, Penicillin G Procaine Allergy, Anaphylactic Shock Protocol, Allergy Testing Penicillin, Anaphylaxis First Aid, Immediate Allergy Care